Hi Sheel -- thanks for the info. I think, in short, I will nee to be
mindful of open cases as I move forward.
But for now, I have one small follow-up question and then one larger
question about the structure of an application.
1-- The little follow-up question: above, when you point out that what
matters when determining how many cases get downloaded into the phone is
how many cases that USER has access to, it will download all the cases of
all types that that user has rights to, and it doesn't matter if that app
only has the ability to work with one case type. You then say "To figure
out which cases a user will get when logging in, you can use the Case List
report and filter by the user." My question is ... based on what you've
said, when I go to that Case List report and filter by user, I obviously do
not limit that report by the other options that case list report offers:
(A) I will leave that report on "Case Type = All" , correct, because of
what you've said above?
(B) However, this case list report also allows me to choose to view opened
vs. closed cases. Am I right that if cases were fully CLOSED, they would
not be synced to the phone, therefore in simulating the case load using
this report, I should set Opened/Closed to only Open?
2-- Here is my bigger question. My initial version of my HIV outreach and
referrals application, which I've been bugging you about in the thread
above, limited the scope of what CommCare would be tracking so that its
tracking halted the moment that a client successfully appeared at a clinic
to fulfill the referral they had been given by the outreach worker. In
that early version, we did *not *plan to use CommCare to continue to track
the continued engagement of people that went deeper into the clinical
system when they tested HIV Positive and therefore joined an ART program on
a fairly permanent basis and therefore came to the clinic for many visits
over time to obtain this or that treatment or service.
But, in a nutshell, I am now being told that we should extend
CommCare's tracking so that it does do that "fuller reach into tracking the
ongoing services gained through entry into the ART program."
Therefore, I have written up an initial understanding of the way that
CommCare could handle that. In fact I've built that first version and
tested it and it functions. BUT, I could imagine there could be any number
of things about the plan that might raise concerns from you experts, or
that might be less ideal about it.
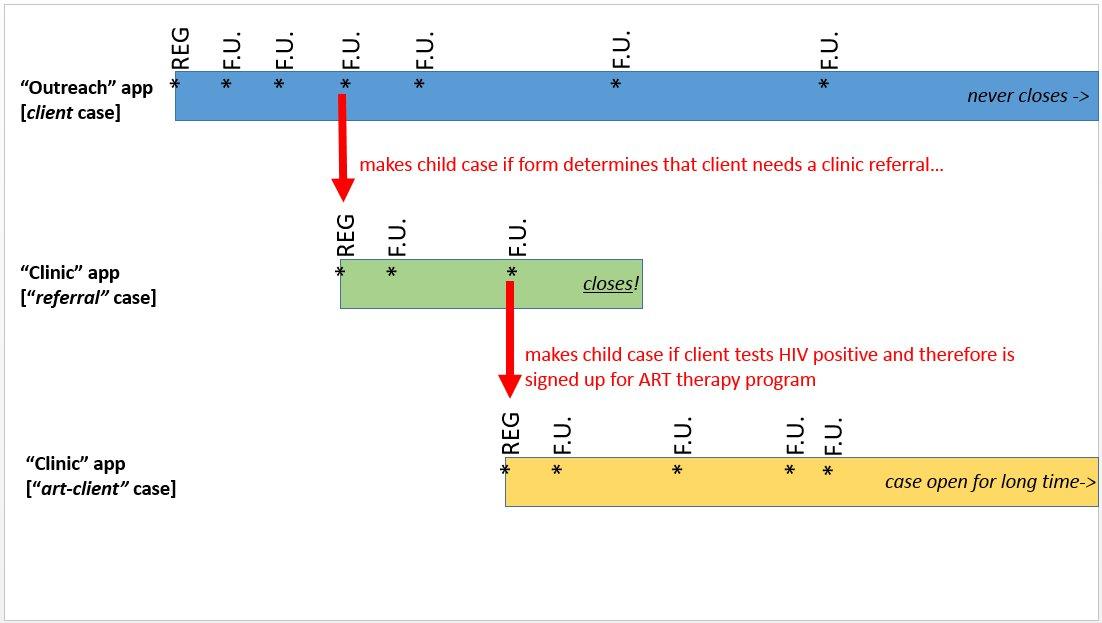
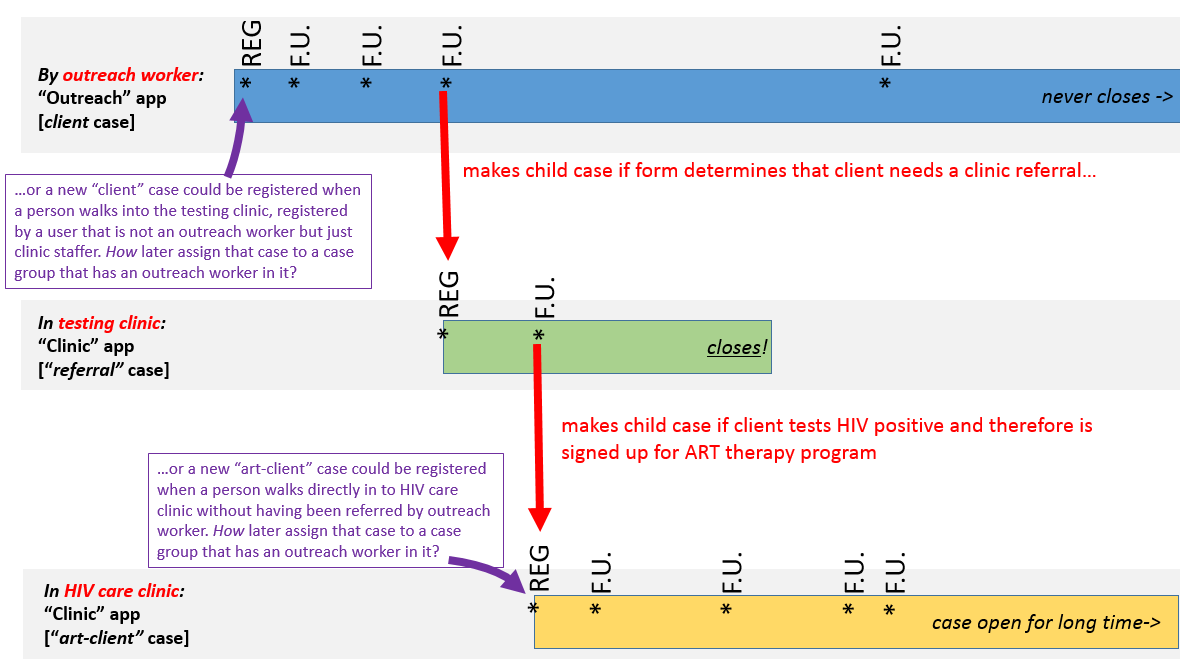
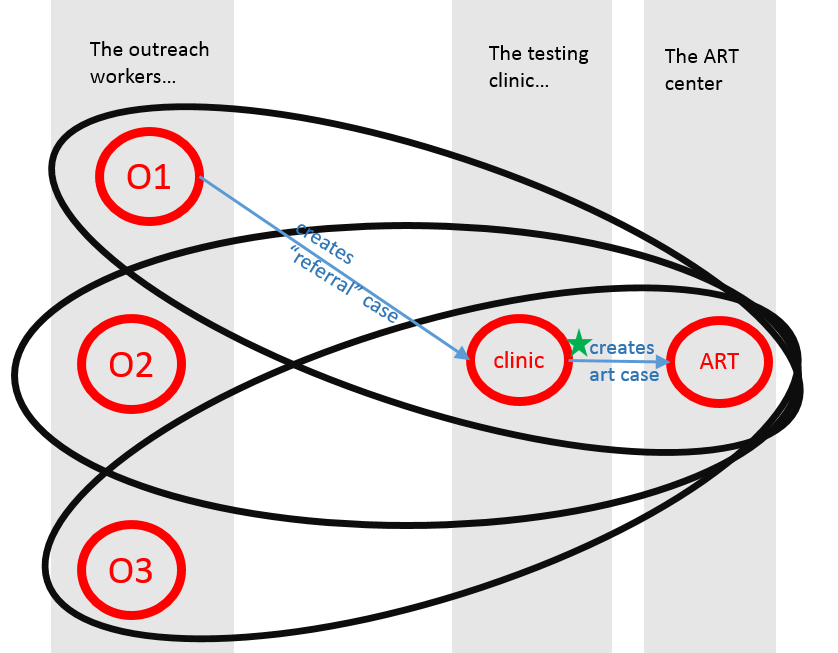
So, could you look at the attached diagram, which shows the method
I've been considering? As you will see, it now has extended into three
case types. The first is for the permanent relationship with an outreach
client over time -- just meeting them in a bar or venue over time, having
screening discussions, etc. The second is for when a referral is made to a
clinic, which is then marked as "completed" if the client successfully
appears (valuable data there.) Now, the new third case type is for IF the
client tests HIV positive and therefore is enrolled in an ART program, the
third case type tracks their ongoing engagement with, and services from,
that program over time.
(A) First of all, what impressions do you have of this plan -- does it make
sense, and any problems or worries rise from it?
(B) Second, I have to admit that it feels cleaner to have broken the
ongoing-ART-program aspect out into its own third case type... BUT, I
wonder if, for the reasons of worrying less about too many open cases, that
it would be smart to combine that ART-program engagement into that second
case type, the regular "referral" case type... so that, if a person tested
HIV negative, then that case would just be closed normally, BUT if the
person tested HIV positive, you would basically keep it open indefinitely
and just start to use that "referral" case type to record the ongoing ART
program participation. Would that be better? If yes, is it emphatically
better, or just mildly? ![]()
(C) What other structure might be best for this goal?
THANKS! --Eric